![]() Back
Back
Virtual Educational Channel
- Virtual Global interactive Staff Meetings around a clinical case
The constraints of the worldwide Covid-19 pandemic require OESO to adapt its educational structure.
A new initiative responds to this need: the OESO-SEMPIRE VIRTUAL EDUCATIONAL CHANNEL.
It is built on the basis, already operational, of the OESO-SEMPIRE Platform ![]()
coordinating the educational activities of a network of Pilot Centers of Excellence in Esophagology worldwide.
Like many of the previous ones, this approach is original, multi-disciplinary, and, from the outset, global.
Its implementation is made possible by use of the virtual techniques of communication available today.
Each time, one of the Pilot centers will propose a challenging clinical case open for interactive discussion, followed by the commentary of an invited expert.
The topic and time will be announced well in advance on the OESO website, with specification of the time to allow connection at a comfortable hour of the day.
Join us,
for an innovative series of international "Staff meetings" with experts from the five parts of the world.
The OESO-SEMPIRE virtual channel will welcome, in addition to the Pilot Centers of the network
able to connect, the contribution of
- all the members of OESO,
- other renowned specialists bringing their specific knowledge into the network, whatever their discipline,
- and, more widely, members of the international scientific community.
- Setting up a meeting
Specifications:
- Transmitted from one of the Pilot Centers of the OESO-SEMPIRE Platform.
- Intended for Pilot Centers in another part of the world, taking into account the time differences.
- Chaired by the Scientific Director of the Center with a member of the junior faculty.
- Short duration: 1-2 hours.
Content:
- Presentation of a challenging case in esophagology, preferably involving several disciplines,
– Exchange of views between the presenters,
– Discussion with people connected in another part of the world with their audience
(prior announcements made by the Centers to encourage attendance). - Invited commentary given by an internationally recognized expert who can also contribute his/her experience to the panel discussion.
These experts don't have to belong to the OESO-SEMPIRE network.
Technology:
- Zoom type technology,
- with announcement well in advance requiring prior signing up of potential participants.
- Courses and discussions recorded and available on the OESO website.
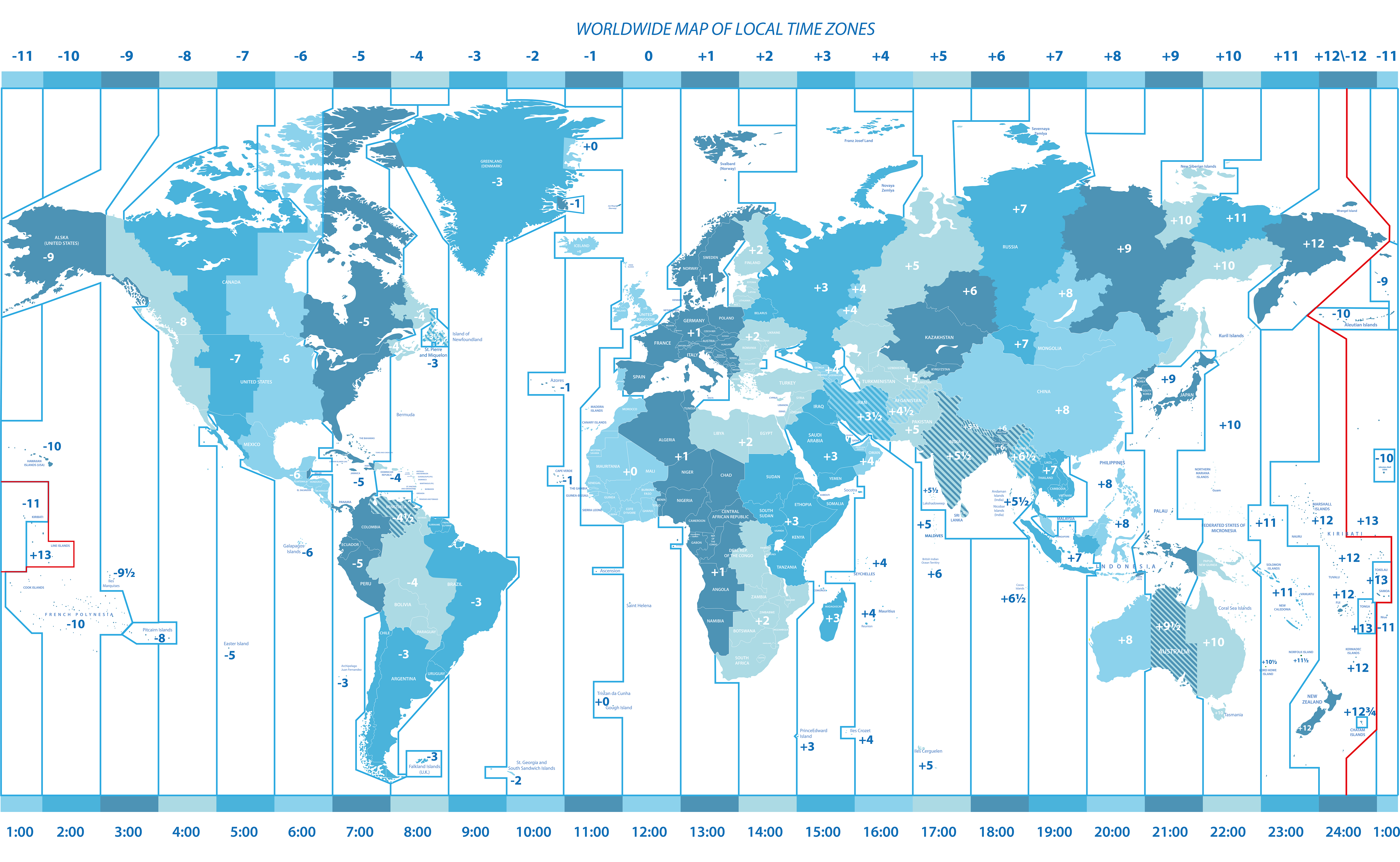
- Time zones > Chart download pdf

Each Pilot Center to choose a preferable time (7-9 am or 5-7 pm) for its program
and know the corresponding time for other Centers wishing to attend the meeting.
Calendar
*
26th meeting
Harvard Medical School, Brigham and Women's Hospital,
and VA Boston Health Care
Hosted by
Walter W. Chan and Hiroshi Mashimo
Thursday, March 23, 2023
- North America – Eastern time: 3 – 5 pm
- Europe CET: Paris: 8 – 10 pm / UK: 7 – 9 pm
- North America: West Coast: 12 noon – 2 pm / East Coast: 3 – 5 pm
- South America: São Paulo: 4 – 6 pm
- Africa: Bomet, Kenya, 10 pm – 12 midnight
- Asia: Malaysia, Kuala Lumpur: 3 – 5 am (Mar. 24) / Beijing: 3 – 5 am (Mar. 24)
- Australia: Melbourne: 6 – 8 am (Mar. 24)
Zoom technology applied
Registration is free, but mandatory:
Gist of the case:
Presenter: Mayssan Muftah (BWH/Harvard)
A 68 year-old woman with history of celiac disease and oral lichen planus presents with chronic dysphagia. We will be focusing on the evaluation and management of patients with esophageal lichen planus.
Topics for discussion:
- Clinical presentation and diagnosis
- Topical and systemic immunosuppression
- Surveillance upper endoscopy and screening for squamous dysplasia
- Management of squamous dysplasia and squamous cell carcinoma
- Endoscopic therapy for esophageal pre-malignant/malignant lesions
Panel for discussion:
- Walter W. Chan (BWH/Harvard)
- Hiroshi Mashimo (VA Boston/BWH/Harvard)
- Wai-Kit Lo (VA Boston/BWH/Harvard)
- Hiroyuki Aihara (BWH/Harvard)
- Joshua Sloan (University of Minnesota)
- Daniela Jodorkovsky (Mount Sinai)
Date and details of the April clinical case discussion will be announced on the OESO website and in upcoming Newsletters.
_____________________________
25th (hybrid) meeting
From the University Sains Malaysia
Hosted by
Prof. Yeong Yeh (Justin) Lee
MSGH (Malaysian Society of Gastroenterology Hepatology)
Dr. Hans Mahendran
MUGIS (Malaysian Upper Gastrointestinal Surgical Society)
Sunday, February 26, 2023
Malaysia, Kuala Lumpur time: 2 – 6 pm
- Europe CET: Paris: 7 – 11 am / UK: 6 – 10 am
- North America: West Coast: (Feb. 25) 10 pm – 2 am / East Coast: 1 – 5 am
- South America: São Paulo: 3 – 7 am
- Africa: Bomet, Kenya, 9 am – 1 pm
- Asia: Malaysia, Kuala Lumpur: 2 – 6 pm / Beijing: 2 – 6 pm
- Australia: Melbourne: 5 – 9 p
Physical venue: Mandarin Oriental Hotel, Kuala Lumpur
Virtual venue: Zoom technology applied, new OESO-SEMPIRE Platform
The 25th meeting presented on the OESO Virtual Channel will be an event:
the launching of the OESO-SEMPIRE Platform for Esophageal Health.
For the first time, the Platform will be technologically put into action, providing access for the international scientific community.
This launching will take place on Sunday, February 26, starting at 2:00 pm (Malaysian time) by representatives of OESO and the Director of Operations of the firm Anderes Fourdy, which will take in charge the technological implementation of the Platform.
During this presentation, a Question and Answer session will highlight the various functionalities that will make the OESO-SEMPIRE Platform a unique tool for dissemination of information and knowledge sharing in all disciplines related to the foregut.
The launching will be followed by a full scientific session organized by two Malaysian Scientific Societies, MSGH and MUGIS, with OESO, illustrating the multi-disciplinary nature of the proposed program.
The single topic, "Disorders of the EGJ outflow" is challenging.
Eminent speakers will discuss its different aspects.
You are invited to show your interest in this new OESO initiative by your presence.
Registration is free, but mandatory:

Program
2 – 2.30 pm – Registration (Physical & Virtual)
2.30 – 3 pm – Introduction from MUGIS & MSGH
Hans Mahendran (MUGIS) & Yeong Yeh (Justin) Lee (MSGH)
_____________________________
Launching of
The OESO-SEMPIRE Educational Platform for Esophageal Health
Robert Giuli (France)
George Triadafilopoulos (USA) – Hiroshi Mashimo (USA) – Yeong Yeh (Justin) Lee (Malaysia)
Nikki Johnston (USA)
Rahul Bharadwaj (Malaysia)
3 – 3.30 pm – Session 1: Who and How should one be tested?
Moderators:
Hiroshi Mashimo (USA) – George Triadafilopoulos (USA) –
Tanisa Patcharatrakul (Thailand) – Justin Lee (Malaysia)
- How to evaluate dysphagia with suspicion of pseudoachalasia or obstructive causes of the EGJ? (5 min) Edoardo Savarino (Italy)
- Disorders of EGJ outflow: how to define? What is the epidemiology? and what are the causes? (5 min) Ying-Lian Xiao (China)
- Is high-resolution manometry good enough to diagnose disorders of EGJ outflow?
(5 min) Prakash Gyawali (USA) - What alternatives are there if high-resolution manometry is unavailable or inconclusive? (5 min) John Clarke (USA)
Q&A (10 min)
3.30 – 4 pm – Session 2: Diagnostic dilemmas and conundrums
Moderators:
John Clarke (USA) – Ellen Stein (USA) – Tee Sze Chee (Malaysia)
- Case 1 (5 min) Phei Oon Tan (Malaysia)
- Case 2 (5 min) Kee Huat Chuah (Malaysia)
- Case 3 (5 min) Tanisa Patcharatrakul (Thailand)
- How does manometry phenotyping help in determining the prognosis of disorder of EGJ outflow? (5 min) Walter Chan (USA)
Q&A (10 min)
4 – 4.10 pm – Break: Video of the new OESO-Sempire Platform
4.10 – 4.40 pm – Session 3: Surgical management
Moderators:
Stefan P. Monig (Switzerland) – Kenric M. Murayama (USA) –
Hans Mahendran (Malaysia)
- Case 6 (5 min) Lau Peng Choon (Malaysia)
- Case 7 (5 min) Renata Vianna Soares (USA)
- Should myotomy always combine with anti-reflux procedure? (5 min)
Hon Chi Yip (Hong Kong) - What is recommended for refractory or failed initial therapy? (5 min) Roger Tatum (USA)
Q&A (10 min)
4.40 – 5.10 pm – Session 4: Non-surgical management
Moderators:
Raman Muthukarappan (Malaysia) – Rona Lawenko (Philippines) –
Sanjiv Mahadeva (Malaysia)
- Case 4 (5 min) Shiaw-Hooi George Ho (Malaysia)
- Case 5 (5 min) Ping-Huei Tseng (Taiwan)
- What are the primary aims of treatment outcome in disorders of EGJ outflow? (5 min)Kristle Lynch
- When do I choose pneumatic dilation over POEM in disorders of EGJ outflow? (5 min)Ellen Stein (USA)
Q&A (10 min)
5.10 – 6 pm – Tea Break (including soft launch of the local consensus)
*
23rd meeting (new date):
From the University of Stanford, California, USA
Hosted by John O. Clarke
Wednesday, January 11, 2023
North America, West Coast PST, Stanford 7:00- 9:00 am
- Europe CET: Paris: 4 – 6 pm, UK: 3 – 5 pm
- North America: West Coast: 7 – 9 am, East Coast: 10 am – 12 noon
- South America: São Paulo: 12 noon – 2 pm
- Africa: Bomet, Kenya, 6 – 8 pm
- Asia: Malaysia, Kuala Lumpur: 11 pm – 1 am (Jan. 12), Beijing: 11 pm – 1 am (Jan. 12)
- Australia: Melbourne: 2 – 4 am (Jan. 12)
Gist of the case:
Presentation of the case by the Stanford group
A healthy 50s year old man with a diagnosis of achalasia.
Focusing on his initial management options and subsequent steps
when those are only transiently successful.
Topics for discussion: this patient is facing management decisions.
- focus on diagnosis tests,
- choice of initial therapy,
- next steps in therapy,
- practicalities of changing management over time,
- technical challenges in re-do procedures
Panel for discussion:
- John Clarke, George Triadafilopoulos, Afrin Kamal, Shai Friedland (Stanford)
- Ellen Stein (Rutgers University, New Brunswick)
- Roger Tatum (University of Washington)
- Eun Ji Shin (John Hopkins, Baltimore)
- Y.Y. Justin Lee (University Sains, Malaysia)
*
24th meeting:
From the OESO-SEMPIRE Pilot Center of Geneva
department of Visceral Surgery
Hôpitaux Universitaires de Genève (HUG)
Hosted by Prof. Stefan Paul Mönig
Head of Upper GI Surgery
Wednesday, December 14, 2022
Geneva, 5 – 7 pm – Europe CET
- Europe: Paris: 5 – 7 pm / UK: 4 – 6 pm
- North America: West Coast: 8 – 10 am / East Coast: 11 am – 1 pm
- South America: São Paulo: 1 – 3 pm
- Africa: Bomet, Kenya, 7 – 9 pm
- Asia: Malaysia, Kuala Lumpur: 12 midnight – 2 am (Dec. 15) /
Beijing: 12 midnight – 2 am (Dec.15) - Australia: Melbourne: 3 – 5 am (Dec. 15)
Registration is free, but mandatory:
Gist of the 1st case:
Presentation of the case: Dr Mickaël Chevallay
Management of giant hiatal hernias – Robotic approach
A 81 year old patient with reflux, dysphagia and anemia.
Diagnosis of a large type III hiatal hernia confirmed by abdominal CT-Scan.

Topics for discussion:
- Which pre-operative tests are important?
- Minimally invasive approach? Laparoscopic versus robotic?
- Mesh or no mesh?
Gist of the 2nd case:
Presentation of the case: Dr Camille Brasset
How to manage hiatal hernias after esophagectomy
A 43-year-old patient, known for a post esophagectomy status for a squamous cell esophageal cancer in 2019.
Emergency admission for pain and vomiting after a paragliding flight.
Diaphragmatic hernia with colic content confirmed by CT-Scan.

Topics for discussion:
- How to close the defect?
- Minimally invasive approach?
- Mesh or no mesh?
- Preventive measures?
Panel for discussion:
- D.E. Azagury (Stanford)
- M. Chevallay (Geneva)
- P. Grimminger (Mainz)
- C. Gronnier (Bordeaux)
- M. Jung (Geneva)
- S. Mönig (Geneva)
- B. Müller (Basel)
- S. Schoppmann (Vienna)
- A. Simic (Belgrade)
- R. Tatum (Seattle)
- D. Van der Peet (Amsterdam)
- J. Zehetner (Bern)
The next, 25th clinical case discussion will be organized on January 2023,
from Stanford by John O. Clarke.
Date and details on time will be announced on the OESO website and in next Newsletters.
***
23rd meeting: postponed to January 11, 2023
From the University of Stanford, California, USA
Hosted by John O. Clarke
Wednesday, November 30, 2022
North America, West Coast PST, Stanford 7:00- 9:00 am
- Europe CET: Paris: 4 – 6 pm, UK: 3 – 5 pm
- North America: West Coast: 7 – 9 am, East Coast: 10 am – 12 noon
- South America: São Paulo: 12 noon – 2 pm
- Africa: Bomet, Kenya, 6 – 8 pm
- Asia: Malaysia, Kuala Lumpur: 11 pm – 1 am (Dec. 1), Beijing: 11 pm – 1 am (Dec. 1)
- Australia: Melbourne: 2 – 4 am (Dec. 1)
Gist of the case:
Presentation of the case by the Stanford group
A healthy 50s year old man with a diagnosis of achalasia.
Focusing on his initial management options and subsequent steps
when those are only transiently successful.
Topics for discussion: this patient is facing management decisions.
- focus on diagnosis tests,
- choice of initial therapy,
- next steps in therapy,
- practicalities of changing management over time,
- technical challenges in re-do procedures
Panel for discussion:
- John Clarke, George Triadafilopoulos, Afrin Kamal, Shai Friedland (Stanford)
- Ellen Stein (Rutgers University, New Brunswick)
- Roger Tatum (University of Washington)
- Eun Ji Shin (John Hopkins, Baltimore)
***
The OESO Zoom Conference
In addition to the discussions organized each month on its Educational Channel,
and in order to compensate for the postponement of its 16th World Congress imposed by the Covid pandemic,
OESO has offered the scientific community a multi-disciplinary alternative of high scientific level.
This conference has been organized by Professor Stefan Mönig and his team, leaders of the
Geneva Pilot Center on the OESO-SEMPIRE Platform of Excellence in Esophagology.
October 28, 2022
Geneva, 1 – 6 pm (CET)
The multi-disciplinary scientific program has involved specialists from different parts of the world.
It is available here ![]()
***
22nd meeting:
From the Department of Surgery, Hospital José Joaquin Aguirre
Faculty of Medicine, University of Chile
Hosted by Italo Braghetto, MD, FACS (Hon), FASA (Hon)
Professor of Surgery
Saturday, October 8, 2022
South America, 9.30 – 11:30 am, Chile
- Europe CET: Paris: 2:30 – 4:30 pm / UK: 1:30 – 3:30 pm
- North America: West Coast: 5:30 – 7:30 am / East Coast: 8.30 – 10:30 am
- South America: São Paulo: 9:30 – 11:30 am
- Africa: Bomet, Kenya, 3:30 – 5:30 pm
- Asia: Malaysia, Kuala Lumpur: 8:30 – 10:30 pm / Beijing: 8:30 – 10:30 pm
- Australia: Melbourne: 11:30 pm – 1:30 am (Oct. 9)
An esophago-tracheal chronic fistula
Gist of the case:
Presenter of the case: Dr Juan Carlos Molina MD FACS
- 55 years, female, no weight loss
- Chronic cough from infancy
- Food regurgitation and acute episode of cough only after swallowing
- Never surgical procedure on the neck
- Never radiation
- Never prolonged intubation
- Never caustic injury or trauma
Topics for discussion
Tests to be carried out,
Final diagnosis,
Therapeutic options,
Surgical options, approach and procedures,
Prognosis
Panel for discussion:
- Lorenzo Ferri (Canada)
- Luigi Bonavina (Italy)
- Bruno Zilberstein (Brazil)
- Fauze Maluf (Brazil)
***
21st meeting:
From the Airway Reflux
OESO-SEMPIRE Pilot Center Medical College of Wisconsin
Milwaukee, Wisconsin
Hosted by Nikki Johnston, Ph.D.
Professor of Otolaryngology and Communication Sciences
Director of Airway, Digestive and Voice Research Education Coordinator
Friday, September 23, 2022
North America, 9 – 11 am Wisconsin / CDT
- Europe CET: Paris: 4 – 6 pm
- North America: West Coast: 7 – 9 am / East Coast: 10 am – 12 noon
- South America: São Paulo, 11 am – 13 pm
- Africa: Bomet, Kenya, 5 – 7 pm
- Asia: Malaysia, Kuala Lumpur 10 pm – 12 midnight
- Australia: Melbourne, Sat, 24 Sept, 12 midnight – 2 am
Airway Reflux: Is it acid, non-acid, something else?
Perspectives from Laryngology, Gastroenterology, Respiratory Medicine, Surgery, and Research.
Didactic presentation
Pepsin: molecular pathophysiology and diagnostic utility
Tina Samuels, MS, Program Manager
Gastroesophageal and extraesophageal reflux are prevalent and costly diseases. Recognition of the pathogenicity of nonacid reflux has stimulated interest in alternatives to acid-targeting diagnostics and therapeutics. Pepsin is the most deleterious enzyme in refluxate, eliciting inflammatory and carcinogenic effects irrespective of acid. Its presence in all refluxate and detection in saliva have situated pepsin as the most widely researched biomarker for reflux today. A summary of the emerging findings regarding pepsin-mediated damage during reflux and developments in pepsin-targeting diagnostics will be presented.
Didactic presentation
Fosamprenavir for the treatment of Laryngopharyngeal Reflux (LPR)
Nikki Johnston, PhD
Given the paucity of data supporting efficacy of acid-suppression therapy for laryngopharyngeal reflux (LPR), the America Gastroenterology Association recommends against its use in the absence of classic gastro-esophageal reflux disease (GERD) symptoms. With compelling evidence of nonacid proximal reflux of pepsin and its association with laryngeal and pharyngeal symptoms and endoscopic findings, a new treatment which specifically targets pepsin could be of great value. Fosamprenavir was found to bind to and inhibit pepsin, abrogating pepsin-mediated laryngeal inflammation and mucosal damage in an LPR mouse model. Fosamprenavir has a good safety profile, is well-tolerated, and targets a foreign virus, making it an ideal drug to repurpose/reformulate, allowing a more expeditious and limited safety assessment in a clinical trial compared to a new molecule. Furthermore, this new approach would be amenable to local treatment of readily accessible airways affected by LPR allowing lower dosing, limiting systemic side effects. FDA/IND approval has been obtained for a 12-week, randomized, placebo-controlled, double-blind, phase III clinical trial to assess the efficacy of oral fosamprenavir for the treatment of LPR. Safety, tolerability, and pharmacokinetic parameters of fosamprenavir administered by dry powder inhaler is also being assessed.
Case 1:
Presenter: Prof. Jonathan Bock
Medical College of Wisconsin
46 year old male financial analyst with many years of allergy and cough symptoms
- History of allergy shots, PFT’s with variable inspiratory phase
- Longstanding spells of sudden SOB with exertion
- Cough, throat clearing, and globus specifically after meals
- No dysphonia, no dysphagia, no sig heartburn or reflux
- DeMeester score 9 but had 98 proximal reflux impedance events, 2 pH positive pharyngeal events, did well on Gaviscon Advance
- Eventually referred for Linx procedure
______________
Case 2:
Presenter: Prof. Thomas L. Carroll
Director, BWH Voice Program, Brigham and Women's Hospital, Harvard Medical School
Chronic cough with talking trigger in a patient with vocal fold paresis and voice change and classic GERD symptoms
38 year old female with 3 years of chronic cough and voice change. She underwent traditional empiric treatments for acidic reflux after negative allergy and asthma workup. Reflux testing off acid suppression confirmed distal acid after BID PPI failed. Vocal fold paresis and glottic insufficiency appreciated on laryngovideostroboscopy. Vocal fold augmentation relieved the cough.
______________
Case 3:
Presenter: Prof. Alyn Morice
Head, Cardiorespiratory Studies, Castle Hill Hospital, Hull York Medical School, UK
34 year old female with chronic cough
- 1967 born
- 1988 chronic dry cough
- 2009 gastro-oesophageal reflux (heartburn and cough)
- 2011 Manometry (St Elsewheres) Hypotonic LO(E)S. “Motility within normal limits”
- 2012 (March) Nissen fundoplication (St Elswheres) peptic symptoms improved. Still coughing
- 2012 (October) seen in the Hull Cough Clinic, HARQ score 45 out of 70
- Trials of promotility agents, azithromycin, metoclopramide, domperidone, baclofen unsuccessful initially a good response to slow release morphine and chlorpheniramine.
- 2014 hiatus hernia on endoscopy
- 2019 referred back to Hull cough clinic. Prominent features voice change, metallic taste, cough on phonation, and the post-prandial cough at 10 minutes.
- Drug trials of P2X3 antagonists and NK1 antagonist without success
- 100% ineffectual. Normal LO(E)S, but HH.
- De Meester 27.38
- Esophageal diverticulum plus HH and dysmotility.
- MTD – proceed to surgery
- 2019 redo Nissen fundoplication, recurrent for large paraoesophageal hiatus hernia, no diverticulum. Scarring ++. Repaired using Bio-A reinforcement
______________
Case 4:
Presenter: Prof. Serhat Bor
Chair, Department of Gastroenterology, Ege University, School of Medicine, Izmir, Turkey
27 year old female referred for the evaluation of anti-reflux surgery
She has been suffering because of heartburn, acid regurgitation and especially hoarseness daily for three years. She wakes up with heartburn and cough.
PPI response is less than 50% for all symptoms.
There is no alarm symptom. Upper gastrointestinal Endoscopy shows LA-A esophagitis.
24 h MII-pH monitoring shows “weak acid reflux”. SAP and SI are negative.
High resolution esophageal manometry is normal.
The patient is also consulted by Psychiatry. She diagnosed with somatisation disorder.
Her strong desire for the antireflux surgery was discusssed during the reflux team meeting and refused. She was put on alginate. She refused the neuromodulators at the beginning but convinced. Amitryptillin 10 mg was started and increased to 20 mg. She is in a much better situation now.
______________
Panel for discussion:
- Serhat Bor, Izmir,Turkey
- Joel Blumin, Milwaukee, USA
- Jonathan Bock, Milwaukee, USA
- Thomas Carroll, Boston, USA
- Alyn Morice, Hull, UK
- Edgar Figueredo, Seattle, USA
*
20th meeting:
From the Gut-Brain Pilot Center of Kota Bharu,
University Sains Malaysia, USM Hospital, Kota Bharu
Hosted by Prof. Justin Yeong Yeh Lee
Tuesday, July 19, 2022
Asia: Malaysia Kota Bharu 6 – 8 pm
- Europe CET, 12 noon – 2 pm
- North America: West Coast: 3 – 5 am / East Coast: 6 – 8 am
- South America: São Paulo, 7 – 9 am
- Africa: Bomet, Kenya, 1 – 3 pm
- Australia: Melbourne, 8 – 10 pm
Refractory GERD in Systemic Sclerosis with CREST syndrome.
Can we do more, or nothing more?
Presentation of the case: Prof. Yeong Yeh Lee
Case: A 60 year old lady with diffuse systemic sclerosis and CREST syndrome, suffering from refractory dysphagia. Surgery is considered.
- Upper endoscopy performed in 2017 showed erosive esophagitis and hiatal hernia. Similar findings at endoscopy performed in 2022.
- High Resolution Manometry in 2017 showed hypotensive LES hincter with aperistaltic esophagus. Similar findings at manometry performed in 2022.
- Recent worsening of symptoms despite Esomeprazole 40 mg BID and Itppride 50 mg TID.
- Fundoplication is considered for this patient.
Discussion points:
- Are symptoms attributed to GERD or dysmotility associated with CREST?
- Is there any role for medical therapy to slow down progression or to treat refractory symptoms
- What are the indications for surgery?
Panel for discussion:
- Yeong Yeh Lee, Kota Bharu
- Naveen Ramasami, Kota Bharu
- Gew Lai Teck, Kuala Lumpur
- Reynu Rajan, Kuala Lumpur
- Yinglian Xiao, Guangzhou
- Hiroshi Mashimo, Boston
_____________________
19th meeting:
From St Vincent’s Hospital, Melbourne
and Tenwek Hospital, Kenya
Hosted by: Dr Matthew Read, MBBS, FRACS, PhD
and
Prof Russell E. White, MD, MPH, FACS, FCS(ECSA)
Director of Cardiothoracic Surgery – Tenwek Hospital
Wednesday, May 4, 2022
Australia, Melbourne, 12 midnight – 1:30 am (May 5)
- Europe CET, Paris: 4 – 5:30 pm
- North America: West Coast: 7 – 8:30 am / East Coast: 10 – 11:30 am
- South America: São Paulo, 11 am – 12:30 pm
- Africa: Bomet, Kenya, 5 – 6:30 pm
- Malaysia: Kuala Lumpur: 10 pm – 12 midnight
Topic: Esophageal cancer in young patients
Subtheme: a celebration of the first fellowship between two Pilot Centers of the OESO-SEMPIRE Platform
The discussion will be based around two cases
Presentation of the cases: Dr Matthew Read and Prof Russell E. White
Case 1: a 23-year-old man, originally from East Africa, recently presented to St Vincent’s Hospital in Melbourne with a four-month history of chest tightness, progressive dysphagia and headache. This was subsequently investigated with endoscopy which revealed a cancer at the GEJ. Subsequent staging excluded metastatic disease.



Figure 1 Figure 2 Figure 3
Figure 1: Endoscopic images detailing the GEJ from above
Figure 2: Endoscopic images detailing the GEJ from below
Figure 3: FDG PET avid lesion at the GEJ
Case 2: a 16-year-old male patient presented with an eight-month history of progressive dysphagia, anorexia, and weight loss.
- Despite multiple visits to health facilities and being treated for a range of different ailments, no endoscopy was performed until seven months later.
- There were no associated risk factors, no history of smoking and no alcohol intake. There was also no significant family history of cancer.
- Histology revealed a moderately differentiated adenocarcinoma.
- Following surgery, the patient made a good recovery. However, they subsequently developed an anastomotic stricture which required serial dilatation. During the post-operative period they also required treatment for a bowel obstruction secondary to a band adhesion.
- Patient developed suicidal ideation in association with a major depressive illness and is currently receiving psychotherapy (12 sessions to date).
Discussion points:
- What challenges exist in the diagnosis & management of esophageal cancer in the younger patient.
- Balancing care, quality of life and survivorship. How to tailor the best approach.
- How do cancers between a younger patient and an older patient compare? Are they different entities and should we be more aggressive with our management?
- Management of esophageal cancer in a resource limited environment.
- Highlighting the significance of the first fellowship between OESO Pilot centers.
The discussion will also include the following presentations:
- Surgery for cancer of the GEJ. How I do it. Dr. Yong Li, Thoracic Surgeon of the Beijing National Cancer Center, China.
- Clinicopathological features of GEJ cancer of the younger patient. Assoc Prof Qin Huang, Harvard Medical School / Brigham and Women’s Hospital, Boston.
Panel for discussion:
- Michael Mwachiro (Program Director, Tenwek)
- Dr Guifang Xu, GI Gastroenterologist of Nanjing Drum Tower Hospital, China
- Dr Lei Wang, GI Gastroenterologist of Nanjing Drum Tower Hospital, China
- Dr Yong Li, Thoracic Surgeon of the Beijing National Cancer Center, China
- Assoc Prof Qin Huang, Harvard Medical School, Boston
Registration is free, but mandatory:
The next clinical case coming up for discussion will be proposed in May by the Pilot Center of Stanford.
Date and details on time will be announced on the OESO website and in next Newsletters.
_____________________________________________
18th meeting:
From Brigham and Women's Hospital /
VA Boston Healthcare / Harvard Medical School
Hosted by:
Hiroshi Mashimo, MD, MS, PhD
Director, GI Motility and Advancing Imaging
Walter CHAN, MD, MPH
Director, GI Motility and Physiology
Thursday, March 24, 2022
North America, East coast: 6:30 – 8 am
- Europe CET: Paris: 11.30 am – 1 pm
- North America: West Coast: 3.30 – 5 am
- South America: São Paulo: 7.30 – 9 am
- Africa: Bomet, Kenya: 13.30 – 3 pm
- Malaysia, Kuala Lumpur: 6.30 – 8 pm
- Australia: Melbourne: 9.30 – 11 pm
Case 1:
a 78-year-old male presenting with dysphagia found to have type II achalasia managed with dilation.
- Patient presented with recurrent dysphagia.
- Reportedly had a diagnosis of achalasia at an outside hospital in the past, managed with repeated Botox injections over a few years.
- We repeated high-resolution manometry and timed barium esophagram, and findings were consistent with type II achalasia.
- He underwent an upper endoscopy with functional luminal imaging probe (FLIP) planimetry that showed low distensibility at the lower esophageal sphincter and absent contractility to volumetric distention in the esophageal body.
- Dilation at the lower esophageal sphincter was performed using the EsoFLIP 30-mm balloon.
- A deep, long linear tear was noted post-dilation concerning for full thickness tear/perforation.
- An esophageal stent was immediately placed to cover the linear tear.
- Post-procedure, the patient was observed in the hospital for two days. He remained stable and was able to advance his diet to full liquid prior to discharge without requiring surgery.
Presentation of the case: Mayssan Muftah, MD, Gatroenterology Fellow
Discussion:
- Assessment of patient with achalasia presenting with recurrent dysphagia.
- The anatomy, physiology and physics relevant to achalasia evaluation and management.
- Treatment of patients with achalasia and how to choose therapy.
- Surgical and endoscopic management of post-dilation complications.
Case 2
a 55 year-old with interstitial lung disease referred for pre-surgical assessment for lung transplantation.
- Patient was diagnosed with interstitial lung disease with declining pulmonary function over the years.
- He underwent comprehensive evaluation for lung transplantation.
- He denied esophageal symptoms, including no heartburn, reflux, regurgitation, or dysphagia.
- A high-resolution esophageal manometry was performed as part of routine pre-transplantation esophageal assessment.
Presentation of the case: Mayssan Muftah, MD, Gatroenterology Fellow
Discussion:
- The role of esophageal testing in patients with advanced lung disease.
- Options and selection of diagnostic testing for esophageal assessment in lung transplant patients.
- Management strategies for esophageal dysfunction and reflux to optimize pulmonary and transplant outcomes.
Panel for discussion: members from Harvard Medical School:
- Jennifer Cai (Assoc. Director, GI Motility and Physiology)
- Walter Chan (Director, GI Motility and Physiology)
- Wai-Kit Lo (Assoc. Director, GI Motility)
- Hiroshi Mashimo (Director, GI Motility and Advanced Imaging)
- Mayssan Muftah (Gatroenterology Fellow)
- Ann DeBord Smith (Chief, Bariatric Surgery)
- Jon Wee (Section Chief, Esophageal Surgery)
- Washington University, St Louis
Ahmed Bazarbashi (Interventional Endoscopy)
The next clinical case coming up for discussion will be proposed in April by the Pilot Center of Melbourne, headed by Prof. Matthew Read.
Date and details on time will be announced on the OESO website and in next Newsletters.
_____________________________________________
17th meeting:
Hosted by
Beijing, Shanghai and Guangzhou
OESO-SEMPIRE Pilot Centers
Tuesday, February 22, 2022
Asia: China 8 – 10 pm
- Europe: CET Paris: 1 – 3 pm
- North America: West Coast: 4 – 6 am / East Coast: 7 – 9 am
- South America: São Paulo, 9 – 11 am
- Africa: Bomet, Kenya, 3 – 5 pm Malaysia: 8 – 10 pm
- Australia: Melbourne, 11 pm – 1 am (Feb 23, 2022)
Special address
by Professor Jie He
Director, National Cancer Center (NCC) of China
President, Cancer Hospital
Chinese Academy of Medical Sciences
Case 1
Immunotherapy-induced pneumonia following neo-adjuvant chemoradiation plus PD-1 inhibitor in a patient with locally advanced esophageal squamous cell carcinoma.
A 61-year-old female with a lesion at the lower thoracic esophagus found by gastroscopy in routine check-up. – Squamous cell carcinoma confirmed by biopsy.
Presentation of the case: Hong Yang – Zerui Zhao (Guangzhou)
- EUS and contrast CT scan showed a cT2N1 locally advanced esophageal squamous cell carcinoma.
- Normal respiratory function and diffusion capacity.
The patient signed a consent for participation in a phase II trial (NCT04006041) on feasibility of combination of Toripalimab (PD-1 inhibitor) and neoadjuvant chemoradiation in esophageal cancer.
- Chemoradiation on April 1st, 2021, with
– 44 Gy in 20 fractions over 4 weeks.
– 4 cycles of Paclitaxel with Cisplatin carried out weekly simultaneously.
– 2 doses of PD-1 inhibitor on day 1 and day 22 during the same time.
- Re-do EUS showed tumor shrinkage, but the subcarinal lymph node
(endo-bronchial ultra-sound guided needle aspiration) suggested the existence of several atypical cells tumor metastases suspected.
- Minimally invasive McKeown esophagectomy performed about 8 weeks following completion of neoadjuvant treatment.
- The pathological report showed a pathological complete response with no evidence of tumor in both primary tumor and resected lymph nodes.
The development of pulmonary dysfunction required mechanical ventilation during the first postoperative week, but the symptoms of dyspnea did not remiss following antibiotic treatment. Besides, only mild elevation of white blood cells and procalcitonin was found by several blood tests. A CT scan carried out on postoperative day 15 showed bilateral lung effusion and pneumonia.
Hence, the multi-disciplinary team specialists in our Institute suggested that the patient might be experiencing immunotherapy induced pneumonia.
- Administration of Prednisolone / 10 days resulted in significant remission of the pneumonia showed by CT scan on postoperative day 25.
The patient was discharged on postoperative day 27 and recovered uneventfully in the out-patient visit 6 months after surgery.
Discussion – Moderator: Yousheng Mao (Beijing)
- Yongtao Han (Sichuan) – Jufeng Liu (Hebei) – Yin Li (Beijing) – Zhigang Li (Shanghai) –
Zhen Wang (Beijing) - Stéphane Bonnet (Paris) – Stefan Mönig (Geneva) – Michael Mwachiro (Bomet, Kenya) –
Edoardo DeMoura (Sao Paulo) – Matthew Read (Melbourne)
Summary: Jianhua Fu (Guangzhou)
*
Case 2
Removal of an esophageal foreign body penetrating into the mediastinum by minimally invasive transcervical mediastinoscopy-assisted approach
Background
Ingestion of foreign bodies, especially animal bones, is one of the most common endoscopic emergencies, especially in China. Foreign bodies can be fishbones, pills, capsules, bottle lids and even false teeth. Fortunately, most of them can be easily be removed by skilled endoscopists, thanks to the development of endoscopic techniques. Only 1% or less require surgery, including foreign bodies with sharp-ends which penetrate the esophageal wall, causing esophageal perforations and remaining in the mediastinum space. The perforating esophageal foreign bodies may cause severe complications, including bleeding and migration.
Traditional approach can be surgery through cervical skin incision. However, for foreign bodies which penetrate in the thoracic esophagus (more than 20 cm from incisors), cervical approach may not be effective and surgery through the chest wall would be inevitable.
In our case, instead of a traditional transcervical approach, we tried a novel, minimal invasive approach with the help of a mediastinoscope.
A 65-year-old woman swallowed a fishbone 10 hours before she was admitted to our hospital with substernal pain.
Presentation of the case: Lijie Tan – Zongwei Chen (Shanghai)
- CT scan and EUS showed upper-thoracic esophageal perforation caused by a foreign body, the distal end being at the level of aortic arch.
The foreign body was located outside the esophageal wall and was adjacent to the upper edge of the aortic arch.
- A transparent cap was attached to the front of the endoscope, showing a longitudinal ulcer, about 0.8 cm/length, 20 cm from the incisors.
- A hook knife was used to cut the esophageal wall along the damaged area, and to expose the submucosal and muscular layers.
In spite of careful examination, no foreign body was found. - After hemostasis with hot biopsy forceps, the wound was closed with clips.
Surgery was therefore needed.
The patient was placed in supine position under general anesthesia with bilateral lung ventilation.
- A 5cm incision was made about 1cm lateral to the SCM.
- A lap-protector (FF00707 Hakko Co Ltd, Japan) with matched retractor (Hakko Co Ltd, Japan), each pre-inserted with three E-Z Trocars
- (5-70mm Short Hakko Co Ltd, Japan), was inserted into the cervical incision.
- Carbon dioxide was insufflatted at a pressure of 8mmHg into the mediastinum to enlarge the very limited mediastinal surgical field, and VISERA ELITE II System OTV-S300 with deflectable laparoscope (Olympus Corporation, Tokyo Japan) was used as mediastinoscope to ensure the maximal surgical view for the operator.
- The operator first inserted a LigasureTM Maryland Jaw sealer (Medtronic) held in the right hand into the upper mediastinum under endoscopic vision, and then inserted a suction stick (which also acted as a retractor) held in the left hand set into the upper mediastinum to provide counter traction on the operative field and remove smoke produced by Ligasure.
- Mobilization of the upper thoracic esophagus was then performed, starting from the left and posterior side of the esophagus.
- The tip of the fishbone was found in the mediastinum before reaching the aortic arch, and a dissecting forceps was used to remove the whole fishbone from the mediastinum.
- The incision was closed after a drainage tube was placed in the surgical field.
Discussion
For most cases of esophageal foreign bodies, a gastroscope is effective. However, once penetrating the esophageal wall, the foreign body cannot be found by gastroscope, and surgery is needed.
In this case, referring to mediastinoscope and laparoscope-assisted esophagectomy, we used the minimally invasive transcervical approach with the help of a deflectable laparoscope to remove the foreign body in the mediastinal space
Preoperative workup is crucial, to investigate the location of the foreign body as to the surrounding important tissues and organs or arteries.
Previous reports demonstrated that CT was useful for a precise, definitive diagnosis of an esophageal foreign body, or when complications were suspected.
CT should be performed again before surgery, because of the risk of migration of the foreign body following the previous maneuvers such as EUS, or movements of the patient.
Discussion – Moderator: Zhentao Yu (Shenzen)
- Keneng Chen (Beijing) – Wentao Fang (Shanghai) – Xuefeng Leng (Sichuan) – Liang Dai (Beijing) – Xufeng Guo (Shanghai)
- Stéphane Bonnet (Paris) – Stefan Mönig (Geneva) – Michael Mwachiro (Bomet) –
Edoardo DeMoura (Sao Paulo) – Matthew Read (Melbourne)
Summary: Lijie Tan (Shanghai)
Registration is free, but mandatory:
The next clinical case coming up for discussion will be proposed in March by the Pilot Center of Boston, headed by Prof. Hiroshi Mashimo.
Date and details on time will be announced on the OESO website and
in next Newsletters.
_____________________________________________
16th meeting:
From the Gut-Brain Pilot Center of Kota Bharu,
University Sains Malaysia
USM Hospital, Kota Bharu
Hosted by Prof. Justin Yeong Yeh Lee
Head of GI function & Motility Unit
Thursday, January 20, 2022
Asia: Malaysia – 11 pm (Jan. 20) – 1 am (Jan. 21)
- Europe CET: Paris: 4 – 6 pm
- North America: West Coast: 7 – 9 am, East Coast: 10 am – 12 noon
- South America: São Paulo, 12 noon – 2 pm
- Africa: Bomet, Kenya, 6 – 8 pm
- Asia: Beijing, 11 pm – 1 am (Jan. 21, 2022)
- Australia: Melbourne, 2 – 4 am (Jan. 21, 2022)
Explaining the unexplained in Non-Cardiac Chest Pain
Presentation of the case:
Prof. Justin Yong Yeh Lee
Dr Tan Phei Oon
Dr Seoparjoo Azmel
Gist of the 1st Case:
A 62 year old Iraqi male, first seen in 2016, with no significant past medical history, presented with chest pain, but cardiac workup was normal.
- Initial upper endoscopy likewise normal, but High-Resolution Manometry showing EGJ outflow obstruction.
- Following balloon dilation, chest pain resolved.
- Recurrence of chest pain in 2019.
- Upper endoscopy showed mild erosive esophagitis, and while manometry was normal, pH-impedance indicated reflux hypersensitivity. He was treated with dexlansoprazole, escitalopram and alginate with initial therapeutic response, but chest pain somewhat persisted.
- Manometry, repeated this time with provocative tests, showed an hypercontractile esophagus, treated with Botox injection.
- In addition, a breast intraductal papillary carcinoma was diagnosed in this patient, and managed conservatively with tamoxifen.
- At the time of the last clinic visit in September 2021, the patient was doing well, with only very occasional chest pain.
Discussion: Management of NCCP
Panel for discussion
Local:
- Justin Yeong Yeh Lee, GI motility
- Tai Pei Oon, GI motility
- Seoparjoo Azmel, Pathology
- Kelvin Voon, Surgery
International:
- George Triadafilopoulos, Gastroenterology-Endoscopy (Stanford, USA)
- John Clarke, Gastroenterology (Stanford, USA)
- Udai Chand Ghoshal, Gastroenterology (Lucknow, India)
- Radu Tutuian, Gastroenterology (Bern, Switzerland)
Registration is free, but mandatory.
*
15th meeting:
From the Pilot Center of Geneva
Department of Visceral Surgery,
Hôpitaux Universitaires de Genève (HUG)
Hosted by Prof. Stefan Paul Mönig,
Head of Upper-GI Surgery
Thursday, December 9, 2021
Europe: CET, Geneva, 5 – 6.30 pm
- North America: West Coast: 8 – 9.30 am / East Coast: 11 am – 0.30 pm
- South America: São Paulo, 1 – 2.30 pm
- Africa: Bomet, Kenya, 7 – 8.30 pm
- Asia: Beijing, Midnight 12 – 1.30 am (December 10, 2021)
- Australia: Melbourne, 3 – 4.30 am (December 10, 2021)
(Preliminary presentations)
- Oligometastatic esophago-gastric cancer:
is there still a place for surgery? Dr M. Chevallay (Geneva) - The OMEC Project. Dr T. Kroese (Utrecht)
Two cases of oligometastatic adenocarcinoma of the esophagus
Presentation of the cases:
Dr Mickael Chevallay (Geneva)
Gist of the 1st Case:
A 59 year old male in excellent condition suffering from epigastric pain and weight loss
for 2 months.
- Gastroscopy (April 2020): lesion at the distal part of the esophagus
(35-40 cm from dental arches), developed on Barrett esophagus. - Biopsy: adenocarcinoma, HER-2 negative.
- Staging with thoraco-abdominal PET Scan and echo-endoscopy:
no metastatic disease.
- Neoadjuvant treatment (CROSS protocol), May – June 2020.
- New staging with PET-Scan and Liver MRI: two liver metastases.
Gist of the 2nd Case:
A 58 year old male with tobacco use, chronic obstructive pulmonary disease
and sleep apnea. Dysphagia and hematemeses.
- Gastroscopy (April 2021): lesion at the distal part of the esophagus
(38-42 cm from dental arches). - Echo-endoscopy staging: uT3 N2.
- Biopsy: adenocarcinoma, HER-2 negative.
- Staging with thoraco-abdominal PET Scan: 4 liver metastases.
- Systemic chemotherapy (FLOT protocol), May – June 2021.
- New staging with PET-Scan and Liver MRI: regression of liver metastases.
Discussion: Management of oligo metastases.
Panel for discussion
Local panel (Geneva):
Stefan Mönig
Minoa Jung
Olivier Huber
International multi-disciplinary panel:
T. Goëtze, Surgical Oncology (Frankfurt, Germany)
T. Schmidt, Surgical Oncology (Köln, Germany)
T.E. Kroese, Surgery (Utrecht, Netherland)
R. Langer, Pathology (Linz, Austria)
J. Wendelmayer, Surgery (Verona, Italy)
S. Schoppmann, Surgery (Vienna, Austria)
____________________________________________
14th meeting:
from the University of Bordeaux, France
Hosted by Prof. Caroline Gronnier and Denis Collet
Hôpital HAUT-LEVEQUE, Pessac, France
Monday, November 22, 2021
Europe: CET, Paris, 5 – 7 pm
- North America: West Coast: 8 – 10 am / East Coast: 11 am – 1 pm
- South America: São Paulo, 1 – 3 pm
- Africa: Bomet, Kenya, 7 – 9 pm
- Asia: Beijing, Midnight 12 – 2 am (November 23, 2021)
- Australia: Melbourne, 3 – 5 am (November 23, 2021)
Gist of the Case:
A disabling case of GERD after esophagectomy
A 48 year old female with history of heartburn and episods of dysphagia for 30 years.
46 Kg, 160 cm (BMI 17 Kg/m²)
- HRM (July 2015) Type 2 achalasia.
– 2 sessions of endoscopic dilation: improvement of symptoms, gained 5 Kgs. During the last session, identification of a superficial, 18mm lesion on mid third of the esophagus.
– Pre-operative workup: T1 squamous cell tumor.
– Endoscopic removal planned in June 2015, but failed, due to submucosal fibrosis precluding submucosal dissection.
- Ivor Lewis procedure performed on July 2016 by laparoscopy and thoracoscopy approach.
– Pathology: T1 N0 R0 squamous cell cancer.
– Postoperative course complicated by gastroparesis which delays oral feeding.
– Patient discharged on POD 17.
- October 2016: suffers from repeated vomits, necessitating a naso-gastric tube.
– Endoscopy shows a large gastric ulcer at the site of the staple line.
– Endoscopic dilation of the pylorus.
– Oral feeding stopped and replaced by enteral nutrition by jejunostomy which falls 2 months later.
- January 2017: weight is 45 Kg (+ 2 Kg).
– Endoscopy shows a persistent ulcer with negative biopsies.
– Oral feeding is still very difficult,
– Endoscopic submucosal pylorotomy performed with poor clinical results.
- March 2017: weight is 34 Kg.
– Naso gastro duodenal tube placed for nutrition.
– Enteral feeding associated with a clinical improvement.
- May 2017: weight is 45 Kg.
– Oral feeding possible but still uncomfortable.
She complains of vomiting, reflux and coughing at night. Healing of gastric ulcer.
- March 2018: duodenal diversion performed, with uneventful postoperative course.
- Two months later, stable weight at 44 Kg
– oral feeding possible and sufficient,
– but still regurgitations and episodes of vomits.
The nutritional status does not improve, due to persistent difficulties for feeding.
- June 2020: jejunostomy: 1 liter of enteral nutrition each night, and 3 meals per day.
- July 2021, weight is 49 Kgs, with normal oral feeding.
- Removal of the jejunostomy planned for December 2021.
Conclusion: severe gastroparesis after Ivor Lewis procedure in a patient who suffered from Type 2 achalasia.
Duodenal diversion performed by our team in similar, but less severe situations in 9 patients.
This time, duodenal diversion did not meet our expectations.
Our indications and results will be discussed during the session.
Presentation of the case:
- Denis Collet (Bordeaux)
- Caroline Gronnier (Bordeaux)
Panel of experts for discussion:
- George Triadafilopoulos (Stanford)
- Guillaume Piessen (Lille)
- Richard McCallum (El Paso)
- Bruno Zilberstein (Sao Paulo)
Registration is free, but mandatory.
_____________________________________________
13th meeting:
From the Center for Robotic Esophageal Surgery
University Medical Center, Mainz, Germany
Hosted by Prof. Peter GRIMMINGER FEBS (hon.)
Head, Upper GI Surgery
Tuesday, October 19, 2021
Europe: Mainz, 17 – 19 pm
- North America: West Coast: 8 – 10 am / East Coast: 11 am – 1 pm
- South America: São Paulo, 12 noon – 2 pm
- Africa: Bomet, Kenya, 18 – 20 pm
- Asia: Beijing, 11 pm – 1 am (October 20, 2021)
- Australia: Melbourne, 2 – 4 am (October 20, 2021)
Gist of the Case:
Robotic esophagectomy for locally advanced distal esophageal cancer
A 52 year old man with a locally advanced adenocarcinoma of the distal esophagus.
- Two-month abdominal pain associated with symptoms of gastro-esophageal reflux. Absence of dysphagia.
- Upper gastrointestinal endoscopy: exophytic and ulcerated tumor, not stenosing, extended from 27 cm to 35 cm from upper incisors, occupying 2/3 of the circumference.
- Biopsy: poorly differentiated adenocarcinoma.
- Ultrasound-endoscopy staging: uT3 uN+ (peritumor lymph nodes).
- Thoraco-abdominal computed tomography (CT SCAN): distal esophagus tumor, with peritumor lymph nodes, no distant metastasis.
- PET-CT: positive FDG up-take, distal esophageal carcinoma with no evidence of distant metastasis.
- Tumor markers: CA 19-9 7.2 U/ml; CEA 2.0 U/ml
- Clinical staging: uT3uN+cM0
Discussion at Tumor Board, with indication of neoadjuvant therapy.
- CROSS regimen from 18.01.2021 to 17.02.2021 (36/41.4 Gy).
Radiotherapy was not well tolerated, due to progressive radio-induced esophagitis. The patient therefore required home parenteral nutrition.
Restaging
- Upper gastrointestinal endoscopy: not stenosing exophytic tumor, in partial regression.
Thoraco-abdominal computed tomography (CT SCAN):
regression of the esophageal parietal thickness.
No evidence of distant metastasis.
Surgical treatment decided at Tumor Board meeting:
- Robotic assisted Ivor-Lewis esophagectomy with 2-field lymphadenectomy
- Uneventful post-operative period. Patient discharged in 8 days.
Final pathology:
- ypT0, ypN0 (0/33), L0, V0, Pn0, R0 (complete histopathological response).
- Clinical, radiologic and endoscopic follow up with no evidence of recurrence or distant metastasis so far.
Presentation of the case:
- Prof. Peter Grimminger (Mainz)
Discussion points:
- The role of totally robotic assisted surgery in the treatment of locally advanced tumors of distal esophagus,
- Tailored treatment of advanced esophageal carcinoma.
Panel of experts for discussion:
- Philip Chiu (Hong Kong)
- Klaus Emmanuel (Salzburg)
- Caterina Froiio (Milan)
- Magnus Nilsson (Stockholm)
- Richard Van Hillegersberg (Utrecht)
Registration is free, but mandatory.
_____________________________________________
12th meeting:

At the time of the tremendous Asian Pacific Digestive Week (APDW)
(Kuala Lumpur, August 19-22),
OESO has been invited to organize a particular session which, in the scientific program of this big event, would take place respecting the original, specific OESO format of sharp questions followed by replies in no more than 5 minutes each.
The Congress organizers have made it possible for OESO to have a virtual booth in the virtual exhibit of the Conference.
You will find below the brochure OESO has drawn up for this occasion: it offers a very brief synthesis of the history of our Organization and, especially, its prospects for the years to come.
We hope that you will connect,
- on the following brochure which comprises the program of this OESO session,
- on the APDW website to attend the congress and participate in the discussion.
____________________________________________
11th meeting:
From the Hospital das Clínicas
São Paulo University Medical School, Brazil
Hosted by Prof. Bruno Zilberstein
Professor of Surgery
Wednesday, June 23, 2021
- South America: São Paulo, 10 am – 12 noon
- Europe: Paris, 3 – 5 pm
- North America: West Coast: 6 am / East Coast: 9 – 11 am
- Africa: Bomet, Kenya, 4 – 6 pm
- Asia: Beijing, 9 – 11 pm
- Australia: Melbourne, 11 pm – 1 am (June 24, 2021)
Gist of the Case:
Barrett esophagus
High grade dysplasia
A 65 year old, white male patient.
Non smoker
- Heartburn and regurgitations for 20 years
- No dysphagia, no respiratory symptoms
- Regular use of PPI – 60 m Dexalanzoprazol for the last 3 years
- No weight loss. (BMI = 25 Kg/m2)
Diagnosis process:
- Endoscopy:
2 cm hiatal hernia
C4M6 Barrett’s esophagus (Prague classification)
Nodular area with microvascular patterns alterations - Biopsies: High grade dysplasia in Barrett’s epithelium
- CT scan and Echo-endoscopy: no remarkable findings
Therapeutic process:
- ESD / resection of the lesion and 60% of the columnar epithelium.
- Histology: moderately differentiated adenocarcinoma (T1a)
Invasion till the mucosa
Lateral and deep margins free of adenocarcinoma - Follow-up endoscopy 3 months after ESD:
3 cm hiatal hérnia (Type I)
Ulcer in distal esophagus on the previous site of ESD
Recurrent columnar epithelium in distal esophagus - Biopsies: Barrett’s epithelium with intestinal metaplasia without dysplasia
Surveillance endoscopy planned for 2 months, with biopsies/Seattle protocol,
and RFA ablation of the Barrett epithelium.
Due to COVID 19 pandemic, the patient returned to our department
only after 14 months, complaining of mild dysphagia.
- Endoscopy:
No stenosis
Elevated lesion on the anterior wall of distal esophagus. Biopsies (A)
Ulcer-infiltrative lesion at the right posterolateral wall of the distal esophagus. Biopsies (B)
3 cm hiatal hernia (Type I). - Biopsies:
A: Invasive, moderately differentiated adenocarcinoma at the squamous-columnar junction
B: Poorly differentiated carcinoma at the squamous-columnar junction with intestinal metaplasia and high grade dysplasia in the adjacent columnar mucosa - PET-CT scan: 2-3cm lesion at the GEJ (SUV max 11,2).
No suspicious lymph nodal invasion. - Subtotal esophagectomy with lymphadenectomy and gastric pull-up.
- Histology: poorly differentiated adenocarcinoma at the squamo-columnar junction with intestinal metaplasia and high grade dysplasia in the adjacent columnar mucosa (pT3pN2M0).
Uneventful follow-up:
- Postoperative chemotherapy
- 6 months after surgery, disease-free patient without any complication.
Presentation of the case:
- Prof. Bruno Zilberstein (FMUSP – Brazil)
- Dr Sergio Szachnowicz (FMUSP– Brazil)
Discussion points:
- Diagnosis and management of long Barrett’s esophagus with HGD
- Endoscopic treatment of early adenocarcinoma
- Surveillance after endoscopic treatment of Barrett’s adenocarcinoma
- Siewert type I adenocarcinoma: staging, treatment options, and best practices.
Discussion led by Bruno Zilberstein with a top level panel currently being assembled.
Panel for discussion:
- Italo Braghetto, Santiago de Chile
- Ivan Cecconello, São Paulo
- John Clarke, Stanford
- Yeong Yeh (Justin) Lee, Kuala Lumpur
- Eduardo GH Moura, São Paulo
- Matthew Read, Melbourne
- Rubens AA Sallum, São Paulo
- Andrew Taylor, Melbourne
- David Wang, Dallas
- Yinglian Xiao, Guangzhou
_____________________________________________
10th meeting:
From the IRCCS, Policlinico San Donato, Milan
Hosted by Luigi Bonavina
Professor of Surgery
University of Milan Medical School
Wednesday, May 26, 2021
Europe: CEST Milan, 4 – 6 pm
- North America: West Coast: 7 – 9 am / East Coast: 10 am – 12 noon
- South America: Sao Paulo 11 am – 1 pm
- Africa: Bomet, Kenya 5 – 7 pm
- Asia: Beijing 10 pm – 12 midnight
- Australia: Melbourne 12 midnight – 2 am (Thursday, May 27)
Gist of the Case:
Esophageal achalasia-like motility disorder:
An intriguing clinical scenario and therapeutic implications
- Patient seen in September 2020 with mixed reflux-like and dysphagia,
no weight loss, and nutcracker esophagus. - HRM showing EGJ Outflow Obstruction plus Jackhammer esophagus.
- Differential diagnosis according to the recent Chicago 4.0 classification.
Presentation of the case:
- Luigi Bonavina
- Stefano Siboni (Interactive case presentation-1)
- Pamela Milito (Interactive case presentation-2)
- Emanuele Asti (Surgical implications)
Discussion led by Luigi Bonavina with a top level panel.
Discussion: Therapeutic strategy for a patient with EGJ OO and hypercontractile phenotype:
nifedipine, pneumatic dilation, POEM, Heller myotomy?
Panel for discussion:
- C. Prakash Gyawali, St. Louis MO (USA)
- John O. Clarke, Stanford CA (USA)
- Roberto Penagini, Milan (Italy)
- Robert Bechara, Kingston (Canada)
- Yinglian Xiao, Guangzhou (China)
Registration is free, but mandatory.
The next 11th Clinical case coming up for discussion on June 2021 will be proposed by Prof. Bruno Zilberstein from Sao Paulo.
Details and time will be announced on the OESO website and in the next Newsletter.
_____________________________________________
9th meeting:
Hosted by Prof. Stéphane Bonnet & Brice Gayet
IMM (Institut Mutualiste Montsouris), Paris
Thursday, April 15, 2021
- Europe: CEST Paris, 4 – 6 pm
- North America: West Coast: 7 – 9 am / East Coast: 10 am – 12 noon
- South America: Sao Paulo 11 am – 1 pm
- Asia: Beijing 10 pm – 12 midnight
- Africa: Bomet, Kenya 5 – 7 pm
- Australia: Melbourne 12 midnight – 2 am (Friday, April 16)
- Zoom technology applied
Gist of the Case:
Presentation of the case:
- Stéphane Bonnet (IMM)
- Nicole Faermark (IMM)
A 68-year-old patient, with intermittent dysphagia to liquids and solids,
painful thoracic spasms and intermittent vomiting. Loss of weight around 15 kg.
Diagnosis process:
- CT scan: 5cm long circumferential thickening of the mid thoracic esophagus.
- Endoscopy: pseudo tracheal aspect of the esophagus («trachealization») with multiple rings and no peristalsis.
- Biopsies: normal without eosinophilic esophagitis.
- PET/CT: suspicious 12cm long esophageal fixation (SUV max 15,6).
- Echo-endoscopy: thickening and fusion of wall layers, 36 to 39cm from dental arch.
- High-resolution manometry: impaired relaxation of LES, pan esophageal pressurization pattern.
Therapeutic process:
- After multidisciplinary discussions,
a first series of Botox injections was performed with slight beneficial effect on pain. - Considering the atypical outcome,
a new echo-endoscopy was performed showing a corkscrew aspect of the esophagus and a pseudo diverticulization between 30 to 42cm from dental arch. - Following a new board discussion,
a myotomy, achieved by thoracoscopic approach in prone position, was performed.
Follow-up: Six months later, the patient eats normally, with no pain, and is gaining weight.
Discussion points: the difficult problems of diagnostic and therapeutic approach regarding atypical dysphagia.
- Pre-treatment imaging and endoscopic workup and its interpretation,
- Choice of management (endoscopic or surgical approach),
- Long-term results.
Discussion led by Brice Gayet and Stéphane Bonnet, IMM, Paris
with a top level panel currently being assembled.
Panel for discussion:
- Robert Bechara, Kingston, Canada
- Stefan Mönig, Geneva, Switzerland
- Marcelo Vela, Mayo Clinic, Scottsdale, AZ, USA
- Bruno Zilberstein, Sao Paulo, Brazil
Registration is free, but mandatory.
The next 10th Clinical case coming up for discussion on May 2021 will be proposed by
Prof. Luigi Bonavina from Milan.
Details and time will be announced on the OESO website and in the next Newsletter.
__________________________________________________
8th meeting:
from the University of Stanford
Hosted by by George Triadafilopoulos and John O. Clarke
Friday, March 19, 2021
- Stanford, USA (7:00-9:00 am West Coast PST)
- Europe: 3:00-5:00 pm
- North America: East Coast
- South America: Sao Paulo
- Asia: Beijing 10:00-12:00 pm
- Africa: Bomet, Kenya
- Australia: Melbourne
- Zoom technology applied
Gist of the Case:
Presentation of the case:
- Patricia Garcia (Stanford GI Division)
- Dan Azagury (Stanford Surgery Division)
An obese patient being considered for bariatric surgery and also for future kidney transplant.
EGJ outflow obstruction on manometry and abnormal acid exposure on pH testing.
Concerns on Transplant/Bariatric surgery.
Discussion led by George Triadafilopoulos and John O. Clarke
with a top level panel currently being assembled.
Discussion points:
- Pre-operative physiology testing in bariatric surgery,
- manometric significance of EGJ outflow obstruction.
- The new Chicago classification for manometry, Version 4.
- Reflux & bariatric surgical selection.
Registration is free, but mandatory.
The next 9th Clinical case coming up for discussion on Thursday, April 15, 2021
will be proposed by Prof. Stéphane Bonnet & Brice Gayet, IMM (Institut Mutualiste Montsouris), Paris.
Details and time will be announced on the OESO website and in the next Newsletter.
As of now, you can begin to prepare your own contribution to this interaction,
your thoughts, your questions, and the areas of your experience that need to be better defined.
Robert Giuli, MD, FACS
Professor of Surgery
Founder & Deputy Executive Director of OESO
__________________________________________________
7th meeting:
from the University of Bordeaux, France
Hosted by Prof. Denis Collet
Hôpital HAUT-LEVEQUE, Pessac, France
Thursday, February 25, 2021
- Europe (Bordeaux 5:00 – 7:00 pm CET)
- Africa: Kenya +2h
- North America: West Coast -9h / East Coast -6h
- South America: Sao Paulo -4h
- Asia: Beijing +7h
- Australia: Melbourne +10h
- Zoom technology applied
Gist of the Case:
Presentation of the case: Prof. Caroline Gronnier
A 61 year old male is addressed for a malignant tumour of the EG junction diagnosed during the follow up of a Barrett’s esophagus.
- Mild dysphagia with initial weight loss of 6 Kg, dropped from 94 to 88 Kg.
- Pre-therapeutic workup showing an adenocarcinoma with signet cells extending from the distal third of the esophagus to the upper part of the small curvature (cT3N+M0).
- Pre-operative chemotherapy using the FLOT protocol (4 cycles),
- Total eso-gastrectomy and coloplasty on June 17.
Patient discharged on July 4 after uneventful postoperative course.
Final pathology demonstrated a ypT4aN3R0 adenocarcinoma.
Panel of experts for discussion:
Surgery:
- Prof. Stéphane Bonnet (Pilot Center/Paris)
- Prof. Stefan Mönig (Pilot Center/Geneva)
Pathology:
- Ass. Prof. Maria Westerhoff – University of Michigan – University Hospitals
This case is the opportunity to discuss several problems which are not been resolved so far, concerning the particular cases of adenocarcinomas of the EG junction with signet cells:
- Is preoperative chemotherapy useful, as for the other types of adenocarcinomas?
- How extensive should the resection be, considering the risk of R1 in case of limited resection?
- What are the advantages and disadvantages of coloplasty as a substitute for the esophagus?
These points will be exposed and discussed with a selected panel of the experts.
Registration is free, but mandatory.
__________________________________________________
6th meeting:
from Melbourne, Australia
Hosted by Matthew Read, MD, PhD, MBBS, FRACS
Senior Lecturer, St Vincent’s Hospital, Melbourne
Friday, January 29, 2021
- Africa (Kenya, 10:00 – 12:00 pm)
- North America (El Paso, TX, 1:00 – 3:00 pm)
- South America (Santiago, 5:00 – 7:00 pm)
- Europe (Paris, 9:00 – 11:00 pm)
Zoom technology applied
Gist of the Case:
Recurrent hiatal hernia – Gastric volvulus – Gastroparesis
Presentation of the case: Dr Henry Badgery
A 67 year old lady with an acute gastric volvulus in the setting of a recurrent hiatus hernia.
- The patient had a hiatus hernia repair in a regional country hospital.
- Represented one year later with hernia recurrence and gastric volvulus.
- Transferred to Metropolitan Hospital (St Vincent’s Hospital, Melbourne) for ongoing management.
– Underwent endoscopic decompression and subsequent revisional hiatus hernia repair with 180˚ posterior fundoplication.
Recovered well. - Multiple ED presentations over ensuing months with non-specific gastrointestinal symptoms.
Gastric emptying and gastroscopy suggestive of gastroparesis. - Successfully managed with Botox injection to pylorus.
Panel of experts for discussion:
Surgery: Professor Lee L. Swanström, Scientific Director – I.H.U. – Strasbourg
Gastroenterology:
- Professor Richard W. McCallum, Texas Tech University Health Sciences – El Paso
- Dr Chamara Basnayake, St’s Vincent Hospital – Melbourne
- Professor Hiroshi Mashimo, Harvard Medical School
Discussion points:
- Surgical management of recurrent hiatus hernia.
- Active management of gastric volvulus,
- Investigation and management of gastroparesis following revisional hiatal hernia surgery.
Registration is free, but mandatory.
__________________________________________________
5th meeting:
Thursday, December 10, 2020
- Time: 4:00 – 5:30 pm Geneva time (GMT+2)
- Zoom technology applied
- Zones in a comfortable time to connect to the meeting:
Africa – South America – North America – Europe
Hosted by Stefan Mönig and Minoa Jung (Geneva Pilot Center)
2 cases will be discussed:
Gist of the 1st Case:
Esophageal gastrointestinal stromal tumors –
A surgical treatment guide.
Presentation of the case: Mirza Muradbegovic
Moderator: Peter Grimminger
A 73 year old female patient with a giant gastrointestinal stromal tumor (GIST) of the distal esophagus.
- Two-month dysphagia associated with spasm. Absence of symptoms of gastro-esophageal reflux.
- Upper gastrointestinal endoscopy with ultrasound and fine needle biopsies: submucosal tumor corresponding immunohistochemically to GIST.
- Thoraco-abdominal computed tomography and positron emission tomography confirmed the esophageal tumor size of 7cm.
Surgical treatment decided at Board meeting:
- Subtotal Ivor Lewis hybrid esophagectomy (laparoscopy and right-side thoracotomy) with intrathoracic end-to-side circular eso-gastric anastomosis.
Uneventful postoperative period was uneventful. Patient discharged/10 days.
Histopathology findings were pT3 N0 L0 V0 PN0 RO low-grade distal esophageal wall GIST 6.5 cm, with low mitotic activity (MA) and no mutations of c-KIT and PDGFRA.
Clinical, radiological, and endoscopic patient follow-up.
Total recovery 15 months after esophagectomy without signs of oncological recurrence or functional disorders.
Panel of experts for discussion:
Surgery: Olivier Huber – Minoa Jung – Stefan Mönig – Beat Müller – Ralph Peterli – Johannes Zacherl
Oncology/Gastroenterology: Markus Möhler
Pathology: Rupert Langer
Discussion points:
- With endoscopic/echographic diagnosis of esophageal submucosal tumor of the esophagus would you recommend a biopsy?
- What additional investigations are necessary (CT scan, PET)?
- In which cases is neoadjuvant treatment recommended?
- What would your surgical strategy be for esophageal GIST? Do you propose radical esophagectomy for all cases? What are the alternative surgical options?
- Is systematic lymph node dissection mandatory?
Gist of the 2nd Case:
Patient with severe obesity, gastroesophageal reflux, and gastric metaplasia.
Which operation to offer?
Presentation of the case: Minoa Jung
Moderator: Ralph Peterli
Barrett esophagus and reflux-esophagitis 5 years after laparoscopic sleeve gastrectomy
and Roux-Y-gastric bypass
A 48-year-old male patient of Spanish origin with BMI 38.4 kg/m2, metabolic syndrome, obstructive sleep apnea, depression, and gastroesophageal reflux.
- Esophagogastroscopy (2016): hiatal hernia with gastritis.
Helicobacter pylori infection eradicated at that time.
Consultation at a private practice center specialized in bariatric surgery to discuss options for surgery.
- Gastroscopy: 10-mm Paris Is superficial lesion of the esophagus above the Z-line and 15-mm Paris IIa–IIb lesion at the incisura angularis.
- Biopsies of the incisura: intestinal metaplasia without helicobacter pylori.
- Endoscopic submucosal dissection (ESD) of gastric metaplasia performed at the private center.
- ESD confirmed a moderate intestinal metaplasia with low-grade atrophic gastritis (OLGIM 2, OLGA 1) at the antrum level.
Consultation at the University Hospital for a second opinion on the most appropriate bariatric surgery option.
Panel of experts for discussion:
Surgery: Peter Grimminger – Olivier Huber – Minoa Jung – Stefan Mönig – Beat Müller –
Johannes Zacherl
Oncology/Gastroenterology: Markus Möhler
Pathology: Rupert Langer
Discussion points:
- Are two lesions with moderate-grade gastric metaplasia (at the level of the incisura angularis and at the level of the distal antrum lesser curvature) considered as risk factors for gastric cancer?
- Which bariatric operation to offer?
– Sleeve gastrectomy
– Roux-en-Y gastric bypass
– Roux-en-Y gastric bypass with removal of the excluded stomach
Registration is free, but mandatory.
__________________________________________________
4th meeting:
Thursday, October 29, 2020
- Time: 5:00 – 7:00 pm Beijing time (9:00 – 11:00 am GMT)
- Zoom technology applied
- Zones in a comfortable time to connect to the meeting:
Africa – South America – North America – Asia – Australia – Europe
Hosted by Jie He and Yousheng Mao
China National Cancer Center
Cancer Hospital, Chinese Academy of Medical Sciences
Multidisciplinary Panels for the discussions:
China: Zhentao Yu (Shenzen) – Yongtao Han (Chengdu) – Keneng Chen (Beijing) – Junfeng Liu (Shijiazhuang) –
Qi Xue (Beijing) – Yin Li (Beijing) – Lijie Tan (Shanghai) – Chun Chen (Fuzhou) – Hecheng Li (Shanghai) –
Xiangning Fu (Wuhan) – Zhigang Li (Shanghai) – Shun Xu (Shenyang) – Yong Li (Beijing) – Jianjun Qin (Beijing) –
Hon Yang (Guangzhou) – Zhen Wang (Beijing) – Xuefeng Leng (Chengdu) – Jiagen Li (Beijing)
USA: Andrew Chang (Ann Arbor) Kenya: Russell White (Bomet) Switzerland: Stefan Mönig (Geneva) Germany: Thorsten Götze (Frankfurt) France: Stephane Bonnet (Paris)
2 cases will be discussed:
Gist of the 1stCase:
- A locally advanced esophageal middle thoracic squamous cell carcinoma with metastatic lymph nodes in the right recurrent nerve area.
- cT3N1M0 Stage III AJCC.
- 4 cycles of neoadjuvant immunotherapy combined with chemotherapy applied.
No adverse events. - Minimally invasive McKeown esophagectomy with two-field lymphadenomectomy 4 weeks after neoadjuvant therapy.
- Final pathological diagnosis: ypT0N0M0
Discussion points, with the panel of experts:
- Value of additional PD-1 blockade
- Neoadjuvant therapy
- Combined immunotherapy
- Evaluation of clinical response to treatment
- Indications for surgery in patients with clinically complete response
Gist of the 2nd Case:
- A potentially resectable locally advanced middle thoracic squamous cell carcinoma
- cT3N1M0 Stage III AJCC.
- Neoadjuvant chemoradiotherapy (2 cycles + 40 Gy).
- Poor response with tumor progression.
- Sequential chemotherapy combined with immunotherapy
- Significant response
- Minimally invasive esophagectomy 4 weeks after, with radical tumor resection.
- Final pathological diagnosis: ypT1bN0M0
- Sudden death of unknown cause.
Discussion points, with the panel of experts:
- Neoadjuvant therapy for locally advanced tumors
- Strategy for patients with poor response to chemoradiotherapy
- Indications for combined immunotherapy
- Indications for surgery in such patients
- Preferable surgical techniques after complex neoadjuvant therapy
Registration is free, but mandatory.
____________________________________________________________
3rd meeting:
Saturday, October 3, 2020
Hosted by Russel White and Michael Mwachiro
From Tenwek Hospital (Bomet, Kenya)
Multidisciplinary Panel for discussion:
Matthew Read (Melbourne) – Kumwinder Dua (Milwaukee)
- Time: 7-9 am EAT (East African Time, GMT+3)
- Zoom technology applied
- Zones in a comfortable time to connect to the meeting:
Gist of the Case:
An unusual case of a 6 year old female involving a foreign body lodged in the esophagus for an extended period of time. The case required a multidisciplinary approach between surgeons and endoscopists to provide appropriate initial care for the patient, and for the complications which arose.
The patient complained of a persistent cough of at least three months duration. She had a chest radiograph performed which revealed the presence of a foreign body in the oesophagus at the level of the tracheal carina. Neither she nor her mother recalled the incident of ingesting the foreign body. The child was able to tolerate a normal diet without difficulty. She did not appear to be in any significant distress, but did have a persistent cough.
Upper GI endoscopy revealed a metallic foreign body, firmly wedged in the mid-esophagus. There appeared also to be a trachea-esophageal fistula present in the anterior surface of the esophagus.
Discussion points, with a panel of experts:
- What would you do with this patient?
- What would be your therapeutic strategy?
- How would you proceed surgically?
____________________________________________________________
2nd meeting:
Wednesday, July 22, 2020
Time: 7-9 am PDT (10 am-12 pm EDT / 4-6 pm CEST / 5-7 pm EAT / 10-12 pm CST)
From Stanford, USA
• Hosted by John Clarke, George Triadafilopoulos and Dan Azagury
• Junior Faculty: Micaela Esquivel, Afrin Kamal and Thomas Zikos
Gist of the Case:
A challenging case of achalasia in the context of hypersensitivity and other comorbidities, with dilemmas in treatment and complications thereafter.
One of the most challenging cases of achalasia management that we have seen at Stanford and sure to stimulate conversation.
Discussion points, with a panel of experts
• Physiology of achalasia
• How to choose the initial line of therapy
• Complications after surgical intervention
• Treatment of reflux after achalasia therapy
• When to consider esophagectomy0
• Treatment of belching
• Next steps
• Zoom technology applied
• Centers in a comfortable time zone to connect to the meeting:
North America – South America – Europe – East and South Africa – Asia
____________________________________________________________
Inaugural meeting:
Thursday May 28, 2020
From Milan, Italy, by Professor Luigi Bonavina – Ass. Prof. Emanuele Asti
From Stanford University, Invited Expert: Professor George Triadafilopoulos
Patient case: a long history of GERD – Association of a giant hiatal hernia ![]()
This first concrete achievement of our new virtual project was unanimously applauded. ![]()
Contact
OESO Head Office
2, Bd Pershing
75017 Paris, France
Tel. + 33 (0)1 55 37 90 15
email: michele.liegeon@oeso.org
Follow us
OESO is now active
on social media!
to get the latest on OESO news, announcements, events, and courses, and to let us know your thoughts!

